~Analyzing the impact on treatment under a declared state of emergency〜
Kobe City has built and commenced operation of a coordinated system that collects data on personal medical care, nursing care, health checkups, etc., which had previously been recorded separately for each individual. This system makes it possible to know at first sight who is healthy and who has a disease. It allows us to obtain not only the current information but also previous history. Therefore, we can even expect to predict possible diseases in the future. In Japan, this is the first system to actively utilize data by coordinating residents’ miscellaneous data on person al medical care, nursing care, health checkup, etc.
As the first effort to analyze data using this system, investigation and analysis of the impact of the prevailing novel coronavirus infection on the treatment of angina pectoris and myocardial infarction, which are the major causes of emergency patient transportation, were performed under the declaration of emergency throughout the months of April and May, 2020. The research team led by Associate Professor Fukuda from Kyushu University consequently confir med that patients in need of emergency treatment had been treated appropriately.
1. Healthcare Data Collaboration Across Platforms
(1) Overview
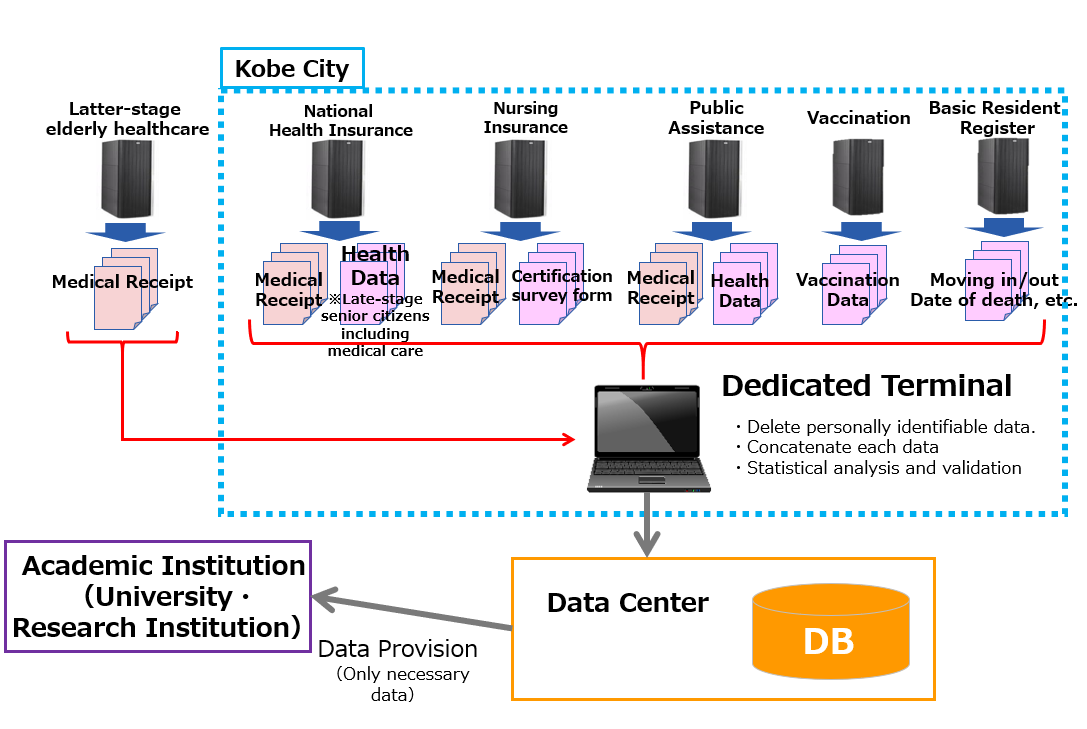
Medical care/nursing care claims data (medical fee/nursing care benefit statements), health checkup data, vaccination data, etc. managed by individual business systems were consolidated on an individual basis by utilizing the data consolidation program developed by Kyushu University.
(2) Data Collaboration Across Platforms
1. Medical Claims Data
Age, Gender, Name of injury or illness, Act of diagnosis, Medical supplies, Medical device, Medical institution, Medical expenses, Number of days to seed Doctor etc.
2. Nursing Claims Data
Age, Gender, Number of nursing care service units by type, Utilization of the intermediate care facilities, Degree of Care, Fee etc.
3. Nursing care certification survey form
Self-sufficiency in daily life, ADL, Degree of care required etc.
4. Medical checkup data
Hight, Weight, BMI、Girth of the abdomen, Blood pressure, Neutral fat, HDL cholesterol, LDL cholesterol, GOT, GPT, γ-GT, Blood sugar level, HbA1c, Urinary sugar, Urine protein, Metabolic Syndrome Assessment, Health guidance level, Living habits etc.
5. Immunization status
6. Move in・Move out・List of date of death etc.
(3) Expected Effects
Availability of comprehensive analysis of more data from past to present on an individual basis will lead to more accurate understanding of the health and lifestyle habits of the residents and promises prediction of possible illness in the future and interpretation of the relationship between lifestyle-related diseases and the need for nursing care.
In addition, it will be possible for us to develop various measures based on scientific evidence, including disease prevention, prevention of aggravation and improvement of vital functions (prevention of frailty), in the fields of health, medical care. For example, interpretation of the relationship between lifestyle-related diseases and the need for nursing care and prediction of the onset of such diseases are expected to allow us to obtain effects, including availability of effective approaches to those who are likely to be in need of nursing care in the future.
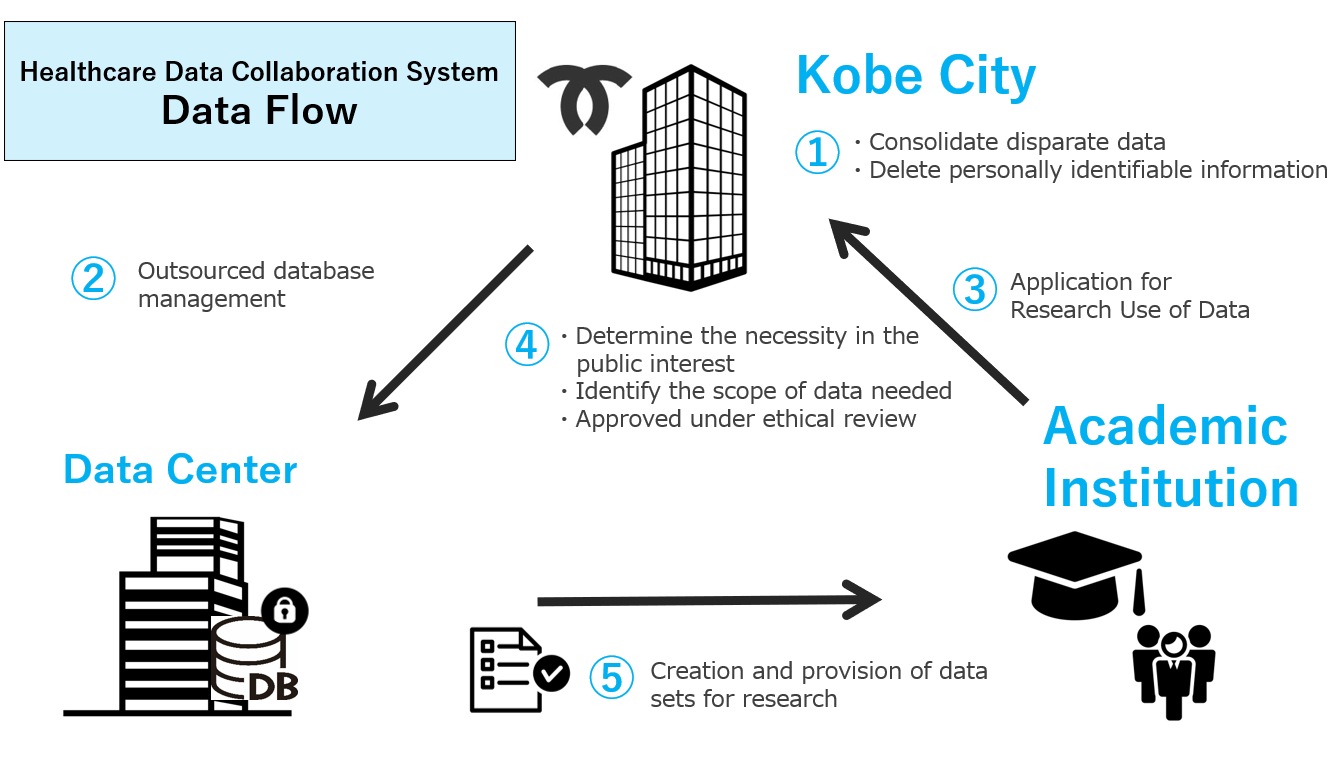
Providing academic institutions with anonymized data for research purposes after predefined procedures and receiving feedback on research results will allow us to obtain advanced knowledge that can be utilized in health promotion measures.
■Image of Healthcare Data Collaboration System
■Flow chart of data provision
2. ”An epidemiological study of the novel coronavirus infection using claims data" (summary of the results)
This research study was conducted by the research group led by Associate Professor Haruhisa Fukuda from Department of Health Care Administration and Management, Graduate School of Medical Sciences, Kyushu University to investigate the impact of the novel coronavirus infection on the treatment of angina pectoris and myocardial infarction, which are the major causes of emergency patient transportation in Japan.
Using medical claims data from Kobe City, the number of percutaneous coronary intervention (PCI) and the changes in the rate of percutaneous coronary intervention (PCI) by categories of urgent and non-urgent heart attacks (angina pectoris and myocardial infarction) were compared between the same months before and after the prevalence of the novel coronavirus infection (in 2019 and 2020).
The results showed that there had been no change in the rate of emergency percutaneous coronary intervention (PCI) in spite of a smaller number of cases of percutaneous coronary intervention (PCI) in total after prevalence of the novel coronavirus infection. It means that only heart attacks not requiring urgent treatment were affected by the prevalence of the novel coronavirus infection. It was confirmed that heart attacks requiring urgent treatment had been properly treated.
In the future, this research study will be continuously conducted, including the analysis of the so-called third wave. Research studies were planned on the effects and side reactions of the novel coronavirus vaccines.
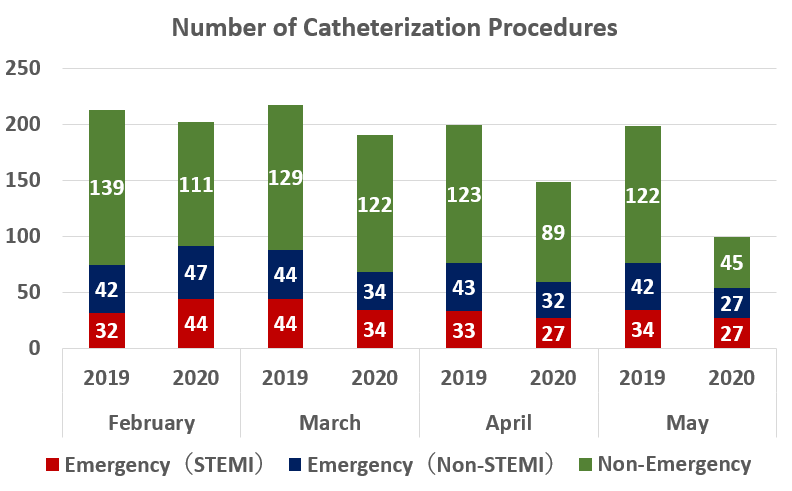
*STEMI: ST-elevation myocardial infarction. Failure of immediate revascularization results in irreversible myocardial necrosis. Therefore, treatment is a race against time in the clinical practice.
*Non-STEMI: non-ST-elevation myocardial infarction This also requires revascularization. However, since non-STEMI does not require greater urgency than STEMI, STEMI and non-STEMI are distinguished in the clinical practice.